Cavernous Sinus Meningioma



Meningiomas involving the cavernous sinus can originate from within the sinus or more typically invade the venous sinus secondarily from other points of origin. These secondary tumors commonly originate from the petrous temporal bone, clivus, clinoid processes, or the lesser wing of the sphenoid.
Meningiomas of the cavernous sinus make up a very small percentage of all cranial meningiomas, but their location within the cavernous sinus makes their surgical resection most challenging. Controversy exists regarding whether surgical intervention for these lesions should even be attempted. This is partially because there is some degree of unfamiliarity with intracavernous surgery and its possibilities.
Historically, the cavernous sinus has been considered a surgical “no man's land” because dissection within its confines often resulted in neurologic morbidity from injury to multiple cranial nerves (CNs), the cavernous internal carotid artery (ICA) or its branches, or this artery's accompanying sympathetic plexus.
However, as microneurosurgical techniques and knowledge of the cavernous sinus anatomy improved, morbidity from surgical resection of these lesions has significantly decreased. This improvement is also a result of more refined indications for surgical intervention.

Atlas Choice Tapered Pattie Collection
Low-profile for maximal visualization and protection
Tapered shape designed for retractorless surgery
Unparalleled flexibility and non-stick features
Clinical Presentation
The presenting symptoms of patients with cavernous sinus meningiomas emanate from the mass effect exerted by the tumor on the neurovascular structures housed within the sinus.
Patients with these tumors typically present with headaches, proptosis due to obstruction of venous outflow, facial pain or numbness, and visual disturbances such as diplopia, anisocoria, ptosis, or scotoma.
Less frequently, they may present with symptoms of carotid stenosis due to mass effect on the ICA. These syndromes include transient ischemic attacks (TIAs), amaurosis fugax, or cerebrovascular accidents (CVAs). Another less frequent presentation includes pituitary dysfunction secondary to mass effect from the meningioma on the pituitary gland or stalk.
Evaluation
The surgeon's evaluation begins with a thorough history, including specific questions about previous surgery or radiation therapy to the area. It is also important to question about involvement of any inflammatory (i.e., sarcoid) and metastatic systemic disease processes with dural involvement that could mimic meningioma on imaging. Nontumorous lesions can readily mimic meningiomas in the cavernous sinus, and their consideration in the differential diagnoses list can have a significant impact on the preoperative workup and ultimately the surgical decision-making process.
Physical and neurologic exams are performed with particular attention to CNs II-VI. This evaluation should also include formal visual field testing to rule out isolated scotomas. A pituitary endocrine evaluation is necessary, including a complete laboratory investigation as is indicated by clinical or radiographic findings, such as mass effect on the hypothalamus or infundibulum.
A MR imaging study analyzes the complex anatomy of the cavernous sinus region. I approximate the origin of the tumor, its degree of cavernous sinus involvement, and abutment of the optic nerve and canal.
MR and CT angiography allow evaluation of the ICA caliber. Any stenosis of the artery implies that the wall of the artery is infiltrated by the tumor and subtotal resection is indicated; the artery should not be manipulated during surgery. Any history of radiation to the cavernous sinus also significantly increases the risk of arterial injury during surgery.
Some of my colleagues advocate for conventional angiography with a balloon test occlusion for patients who have a history of cavernous sinus surgery or radiation or for whom there is significant concern of intraoperative cavernous ICA injury. If poor collateral circulation is demonstrated, they recommend preparation for a high-flow bypass as part of the surgical plan. For more information on this procedure, see the High-Flow Revascularization chapter.
My personal philosophy differs with this recommendation. I do not recommend the use of revascularization to facilitate resection of the infiltrated ICA with the goal of gross total tumor resection. Radiosurgery provides a reliable method for control of small and medium-size residual intracavernous tumors.
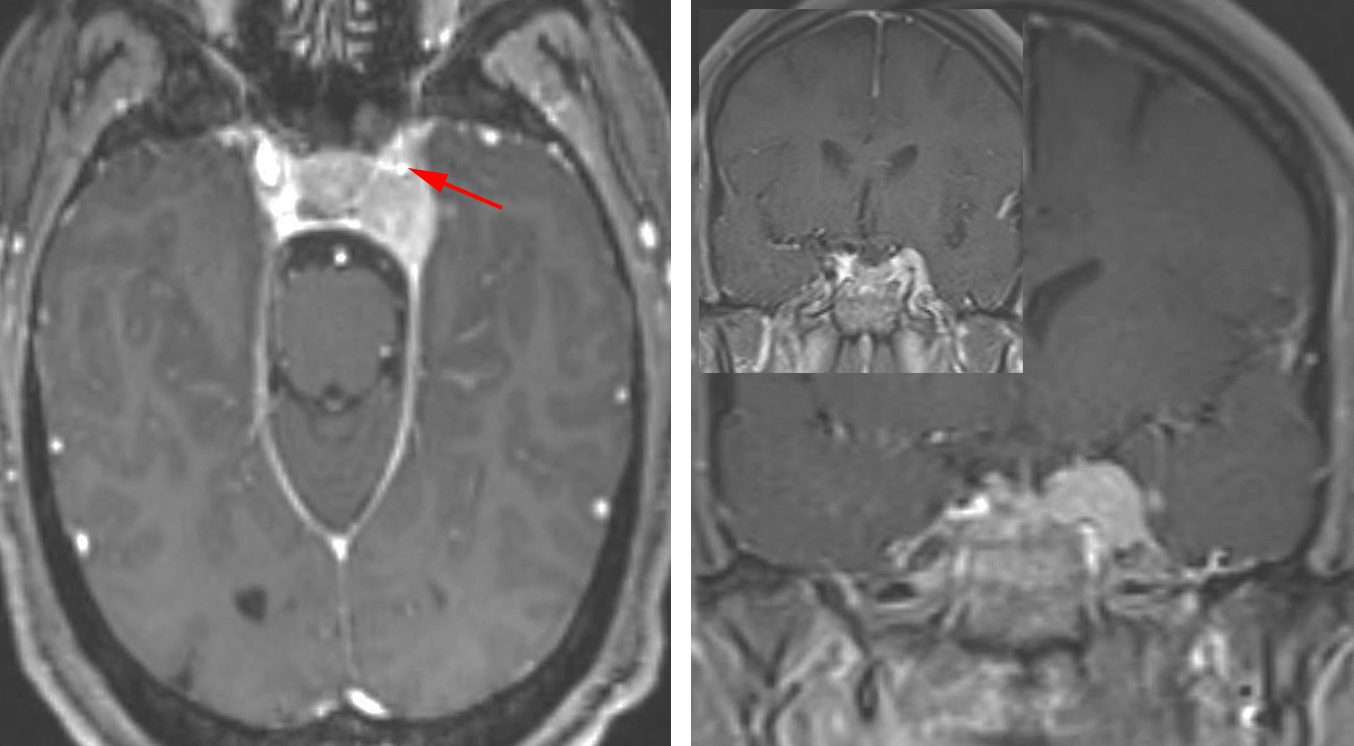
Figure 1: A small left cavernous sinus meningioma is shown. Note the encased and stenosed cavernous ICA (arrow), precluding aggressive dissection around the artery. The mass has pushed the lateral dural margin of the cavernous sinus outward. A dural tail along the edge of the tentorium is also apparent.
Treatment Philosophy
Treatment options for meningiomas include observation, surgical resection, and stereotactic radiosurgery. Most asymptomatic or minimally symptomatic cavernous sinus meningiomas are observed with serial imaging or undergo radiosurgical treatment. A review of current studies supports the finding that more than 60% of patients treated for these tumors harbor quiescent tumors. The recommended follow-up interval for imaging the conservatively managed lesions is at least once a year.
Tumors causing any degree of vision loss due to optic apparatus compression are surgical lesions because vision often improves once the mass effect on CN II is relieved. Documented tumor growth or progressive neurologic deficits are indications for surgical intervention.
Surgical intervention also permits histopathologic diagnosis and grading, which guides future management.
When pursuing surgical intervention, the surgeon must be mindful that the goal is (primarily) safe and (secondarily) near gross total resection during the first operation. Reoperation for these lesions is associated with a high risk of neural and vascular injury.
As previously described, cavernous sinus meningiomas carry a high risk of ICA and intracavernous cranial nerve injury secondary to tumor infiltration of the ICA adventitia and CN perineurium. To prevent injury to these structures, some tumor should be left behind.
Removal of the cavernous sinus meningiomas should focus on safe removal of the extracavernous tumor on the lateral wall of the sinus. I do not attempt aggressive intracavernous tumor resection, particularly in cases where the cavernous ICA is encased (Hirsch grades 2 and 3) and preoperative CN deficits are not present.
The residual tumor can be observed (my preference) or treated with stereotactic radiosurgery (SRS). Increasingly, the combination of planned subtotal resection with SRS is being established as an acceptable paradigm. However, there are limited reports of SRS potentially causing a more aggressive course in patients with late recurrence.
Other studies have shown a recurrence rate of 20% at 20 years following extracavernous resection and conservative intracavernous paradigm. These results suggest the potential efficacy of observation for the residual tumor. Although no consensus exists regarding the best course of action for cavernous sinus meningiomas, I advocate a more conservative surgical strategy with serial imaging to follow residual tumors and radiosurgery in the event of regrowth and recurrence.
Operative Anatomy
The microsurgical anatomy of the cavernous sinus is complex and requires an in-depth study in the laboratory. Intimate anatomic knowledge should be translated from this Atlas to three-dimensional concepts in the cadaver laboratory before its application in the operating room.

Click here to view the interactive module and related content for this image.
Figure 2: The relevant anatomy is demonstrated through progressive, layered, and stepwise extradural dissection of the right cavernous sinus. The lateral wall of the cavernous sinus houses CNs III, IV, V1, and V2, with CN VI passing through the sinus itself by the ICA (left upper photo). The outer layer of the temporal lobe dura has been peeled away from the lateral wall of the cavernous sinus, exposing CNs III and IVentering the roof of the cavernous sinus and passing forward through the superior orbital fissure (right upper photo). CN III enters a short cistern in the sinus roof (red arrow) and does not become incorporated into the lateral wall until it reaches the lower margin of the anterior clinoid process (yellow arrow, left middle image). The remaining dura covering the lateral wall has also been removed (right middle image). The posterior trigeminal root has been reflected forward to expose the posterior part of the lower margin of the cavernous sinus (yellow arrow) in the area medial to the trigeminal impression on the petrous apex (left lower photo). The trigeminal nerve and its three divisions have been reflected forward to expose the venous spaces of the cavernous sinus (right lower image). (Images courtesy of AL Rhoton, Jr.)
The ICA, with its adherent sympathetic plexus, passes through the cavernous sinus and feeds the meningohypophyseal trunk, inferolateral trunk, and occasionally McConnell's capsular artery or a persistent trigeminal artery.
The Hirsch grading of cavernous sinus meningiomas classifies these lesions according to their degree of radiographic involvement of the cavernous segment of the ICA. Hirsch grade 1 lesions come in contact with or partially encase the cavernous ICA. Grades 2 and 3 lesions completely encase the ICA, with grade 2 lesions causing no radiographic narrowing of the ICA lumen and grade 3 lesions causing radiographic narrowing of the artery.
The Hirsch grade serves as an important indicator of the resectability of the tumor. Grade 1 lesions carry the most favorable and grade 3 tumors the least favorable prognosis, due to the requirement for a more aggressive attempt at resection and the correlated higher risk of ICA injury.
This risk can be attributed to the pathologically verified invasion of the adventitia of the cavernous ICA, lacking an intervening arachnoid membrane. Other pathologic studies have shown that meningiomas become continuous with the perineurium of CNs, particularly CN III, accounting for the high risk of injury during aggressive attempts at surgical resection.

Figure 3: Stepwise dissection of the right cavernous sinus from an operative perspective using the extradural approach is shown. The pretemporal orbitozygomatic craniotomy and extradural clinoidectomy are complete and the lateral edge of the superior orbital fissure exposed (left upper photo). The outer layer of the cavernous sinus was separated or peeled off from& its inner layer after cutting the frontotemporal or meningo-orbital dural band at the lateral edge of the superior orbital fissure. The nerves invested in the inner layer of the lateral wall are thereby exposed as the meningeal (outer) layer is peeled away (right upper photo).
After dividing the middle meningeal artery, the peeling continues posteriorly and medially while the greater petrosal nerve is exposed. This nerve usually travels above the petrous ICA and is a good landmark for the artery. The medial edge of the dural mobilization along the middle fossa is at the anterior petroclinoid dural fold, and the posterior edge is at the petrous ridge (left middle image). An enlarged view of the paraclinoid area is also included (right middle image). Note that intradural entry is possible via the Parkinson's triangle. Another view after the inner dural layer of the lateral sinus wall has been removed is shown (left lower photo). The area where the lesion presents into the lateral wall is the point of operative entry. The middle fossa triangles exposed are the anteromedial triangle (between V1 and V2); the anterolateral triangle (between V2 and V3); the posterolateral triangle, also called Glasscock's triangle (between V3 and the greater petrosal nerve); and the posteromedial triangle, also called the Kawase triangle (lateral to the trigeminal nerve and posterior to the greater petrosal nerve). Finally, another view illustrating some portions of the middle fossa floor and roof of the internal auditory canal after bone removed in the area is also included (right lower image). (Images courtesy of AL Rhoton, Jr.)

Figure 4: Another dissection to illustrate similar principles from an intradural perspective is shown. Large tumors are best approached via both intra- and extradural corridors. (Images courtesy of AL Rhoton, Jr.)
RESECTION OF CAVERNOUS SINUS MENINGIOMA
Most cavernous sinus meningiomas are best approached via an orbitozygomatic craniotomy(OZ) and extradural clinoidectomy. This approach is flexible and provides multiple working angles to the entire venous sinus, as well as proximal and distal control over the ICA.
The extended pterional craniotomy and extradural clinoidectomy is also as effective for most tumors (except in the cases of tumors with significant superior and/or middle fossa extension).
As discussed above, the goal of the craniotomy is removal of all extracavernous components of the tumor and conservative excision of the tumor within the lateral-most aspect of the cavernous sinus. If preoperative CN deficits are present, an attempt at these nerves' decompression is justified.
The surgeon should maximize the operative working window by means of liberally removing bone during the approach (i.e., subtemporal craniectomy). I prefer to install a lumbar drain for cerebrospinal fluid drainage to relax the dural sac and facilitate extradural dissection. Cranial nerves III, IV, and VI are monitored during the operation.
For meningiomas within the posterior cavernous sinus, the zygomatic craniotomy or middle fossa/subtemporal craniotomy offers favorable exposure of the posterior cavernous sinus and petrous apex, but suboptimal control over the distal ICA. I do not believe the osteotomy of the zygomatic arch offers significant expanded working angles, and therefore it is superfluous.
The orbitozygomatic osteotomy can be optimally performed with the patient in the supine position and head tilted 30 degrees toward the contralateral side. The patient's neck should be prepared to facilitate proximal carotid artery control.
After the bone flap is elevated, the orbital contents are exposed and electromyographic electrodes are directly placed into the superior oblique, superior rectus, and lateral rectus muscles to monitor CNs III, IV, and VI.

Figure 5: After completion of the orbitozygomatic craniotomy and extradural clinoidectomy, a subtemporal craniectomy is completed so that a direct view of the middle fossa floor is available. The middle fossa dura is then peeled off. The dural sheaths investing V2 and V3 as they exit the floor of the middle fossa are identified and separated from the outer layer of temporal lobe dura. This maneuver allows the extracavernous component of the tumor to be separated from its intracavernous portion extradurally.
Throughout the procedure, I also attempt removal, or at least cauterization, of any infiltrated dura in order to minimize the foci of potential recurrence.
Vascular Control of the ICA
I secure control of the ICA along its full extent (petrous, cavernous, and clinoidal segments) to approximate the location of the ICA engulfed by the artery, avoid inadvertent vascular injury, and minimize the risk of massive blood loss.
To achieve this goal, once elevation of the dura from the middle fossa is complete, the petrous segment of the ICA can be exposed through the Glasscock's triangle. This maneuver is indicated only if aggressive tumor resection is contemplated. The middle meningeal artery is also coagulated and divided during elevation of the middle fossa dura.
Exposure of the ICA is accomplished by first identifying the greater superficial petrosal nerve (GSPN), dividing it, then drilling through the bone with a diamond bit while using copious irrigation. The bone is often dehiscent in this area. Traction on the GSPN is avoided to prevent injury to the geniculate ganglion; such injury can lead to facial palsy.
The apices of the Glasscock triangle are the facial hiatus, the anterior aspect of the foramen ovale, and the intersection of the GSPN and the lateral aspect of the V3. This triangle overlies the carotid artery, and drilling within this triangle using a diamond bit and constant irrigation uncovers the carotid artery.
Proximal control is secured by placement of a temporary clip on the petrous ICA. Alternatively, and more often, a Fogarty catheter is inserted into the carotid canal. When proximal control is necessary, the catheter balloon can be inflated to occlude the carotid artery in the carotid canal.
Distal control is possible by exposing the segment of the ICA between the dural rings. This exposure is achieved by opening the superior orbital fissure.

Figure 6: The uncovering of the carotid artery underneath the Glasscock's triangle and the placement of the Fogarty balloon are demonstrated. Please note that the balloon in placed when the dissection around the carotid artery is undertaken. I do not place the balloon at the beginning of the procedure so it does not interfere with my dissection maneuvers.
Entry into the Cavernous Sinus
If an intracavernous dissection is planned, the sinus can be entered via a superior or a lateral approach, or a combination of the two. Most often, the tumor reaches the surface of the lateral wall of the sinus and guides the surgeon regarding the point of entry.
Moreover, each tumor displaces the intra- and paracavernous sinus structures in a unique way. The operator should use the space created by tumor debulking as the operative route.
Superior Approach
This is an approach for masses near the anterior, superior, and/or medial to the cavernous ICA.
The dura over the optic nerve is incised over the length of the optic canal to untether the optic nerve. Next, the distal carotid ring is divided. The dura is then incised toward the oculomotor nerve, providing initial entry into the cavernous sinus. Exposure can be expanded by additional incisions along and around the carotid artery.
Further exposure can become available via a posterior clinoidectomy and resection of the dorsum sellae. Entry into the posterior fossa is possible. The planum sphenoidale may also be drilled away. Any connection to the nasal sinuses should be sealed off.
Lateral Approach
The lateral approach is favorable for lesions lateral and/or inferior to the ICA and those that are posteriorly located within the cavernous sinus.
Extradural entry begins by incising the dura propria encasing V3. The dura propria is peeled away until the ganglion is in view. The bone around the foramina rotundum and ovale is removed to allow exposure of the infratemporal fossa.
INTRADURAL PROCEDURE
The Parkinson's (infratrochlear) triangle is a reasonable corridor to reach the intradural/intracavernous portion of the tumor. CNs III and IVare found at the edge of the tentorium, and the dural incision is just beneath the route of CN IV. A dural flap is created by extending the dural incision inferiorly and reflecting the flap over the trigeminal ganglion. Tumor mobilization should protect CNVI which often consists of two to five fascicles.

Figure 7: The surgical triangles of the cavernous sinus are illustrated. The tumor often dictates the safe location of entry into the venous sinus. The infra- and supratrochlear triangles are reasonable candidates for entry based on the estimated displacement patterns of the nerves. The anteromedial and anterolateral triangles are other routes necessary for removal of these tumors. Note the location of the Glasscock's triangle for exposure of the carotid artery.
Finally, in the case of tumors with large intradural and suprasellar extension, I incise the convexity frontotemporal dura in standard curvilinear pattern and dissect the extracavernous portion of the meningioma from the brain. The tumor is peeled away from the optic apparatus and pituitary stalk. The parts of the tumor filling the opticocarotid and oculomotor-carotid triangles are also resected.
The surgeon should attempt to remove as much of the infiltrated or hyperostotic bone as safely as possible throughout the resection, decreasing the foci for recurrence.
Within the cavernous sinus, CN VI is identified and protected; stimulation mapping may be used for its localization. Venous bleeding is easily controlled with gentle thrombin-soaked gelfoam packing. Importantly, any traction injury in the nerves is avoided via the use of microdissectors and sharp dissection. Some of these steps are summarized below.

Figure 8: Exposure of the paracavernous area is readily possible via either an OZ osteotomy or extended pterional craniotomy along with extradural anterior clinoidectomy and posterior orbitotomy. For the intradural approach, the extracavernous portion of the tumor is resected first and the optic nerve is decompressed early via opening of the falciform ligament. The extracavernous section of the tumor is devascularized at its based along the medial sphenoid wing dura. The bone around the trigeminal foramina is drilled to expose the portion of the tumor penetrating into the trigeminal foramina.

Figure 9: The components of the tumor affecting the optic nerve are removed first to protect the nerve during the rest of tumor manipulation. Sharp dissection peels off the tumor capsule away from the nerve. Perforating arteries along the inferior surface of the nerve are preserved. Note aggressive devascularization of the tumor at its base and its thorough internal debulking. The temporal and frontal lobes are gently "held in place" and protected via fixed retractors.
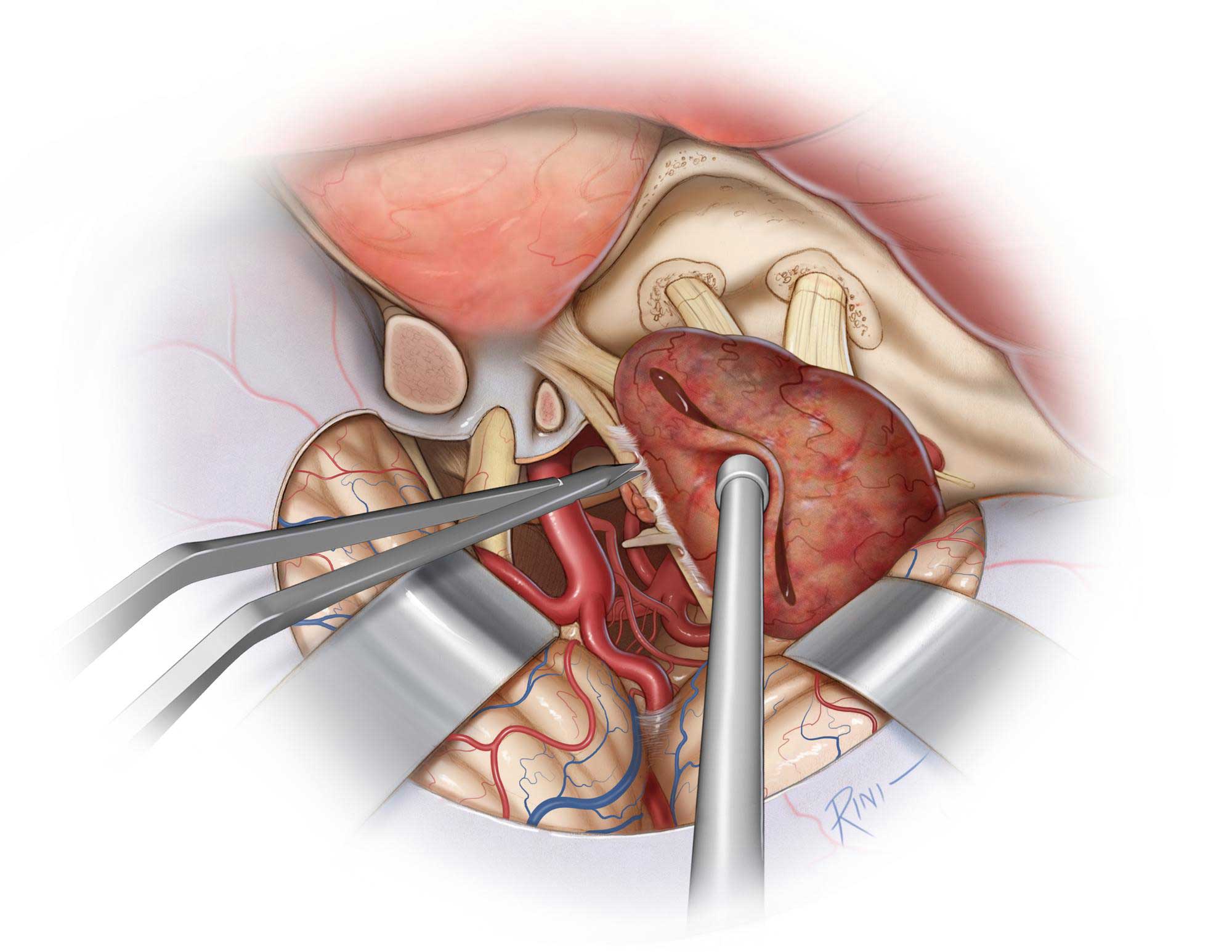
Figure 10: The tumor capsule is continuously mobilized away from the cerebrovascular structures within the opticocarotid cisterns and cranial nerves within the cavernous sinus. Cranial nerve IV is particularly vulnerable to injury during this part of the operation and is identified at edge of the tentorium and followed into the cavernous sinus. Any tumor fragments that are densely adherent to the nerves are left behind to protect function. Perforating arteries in this area are respected.

Figure 11: The tumor is carefully dissected from the Gasserian ganglion. Any portion of the tumor infiltrating the trigeminal foramina is dissected if safely possible. The bony openings around the trigeminal nerve divisions are expanded, if necessary.

Figure 12: A final view of the operative field after tumor resection is illustrated. Small amount of tumor is left around CN IV to avoid permanent morbidity.
Additional Considerations
The spheno-cavernous sinus meningiomas often harbor a dissection plane in proximity to the lateral cavernous wall, thereby allowing more aggressive dissection of the tumor from the neural structures.
If the tumor is infiltrating the Meckel's cave, the dura over the trigeminal ganglion is incised and the tumor is followed posteriorly for its removal. As in the case of other cavernous sinus meningiomas, the tumor creates the most viable, practical, and safe route for its access and removal.
Thick fibrous tumors and those with calcified texture are not safely resectable away from the neurovascular structures.
Case Example
A 54-year-old woman presented with progressive facial numbness.

Figure 13: The images in the top row show the large cavernous sinus meningioma. A right-sided extended pterional approach was selected. Because of the large size of this tumor, a combination of both intra- and extradural routes was used. The lateral wall of the sinus was incised intradurally (second row of images), tumor debulked, and the trigeminal nerves identified (inset image). Upon deflation of the sinus wall, the adherent middle cerebral artery branches were found (third row). Upon near gross total removal of the tumor, CN III was apparent (bottom row of images).
Resection of a Large Cavernous Sinus Meningioma
Closure
Before the bone flap is replaced, the surgical cavity is inspected so that any source of cerebrospinal fluid leakage can be obliterated using pieces of autologous muscle or fat. The area of the clinoidectomy is filled with a small pledget of muscle harvested from the temporalis muscle.
Postoperative Considerations
Patients are typically observed in the Intensive Care Unit for 24 to 48 hours after surgery. The steroid dosage is tapered off within 1 week, depending on the extent of cerebral edema and the patient's neurologic status. Seizure prophylaxis is continued for 7 days postoperatively; if the patient presented with a seizure, seizure prophylaxis is continued for 6 months to a year. Follow-up MRI is obtained within 48 hours of surgery, and once discharged from the hospital, the patient undergoes follow-up 3-month postoperative imaging followed by yearly surveillance imaging for early detection of recurrence.
Cerebrovascular accidents represent a major complication to keep in mind following surgery in the cavernous sinus, but this complication has a relatively infrequent incidence.
The requirement of adjuvant radiation therapy is becoming an important topic of discussion for management of cavernous sinus meningiomas. Use of adjuvant radiation therapy permits a more conservative resection and decreases the rates of postoperative morbidity.
I focus on the use of radiotherapy for treating aggressive local disease, which commonly demands a subtotal resection due to the involvement of critical cavernous sinus anatomy. One important caveat regarding this adaptive approach is the need to sufficiently clear the tumor mass away from the optic nerves/chiasm to allow for the application of higher dose adjuvant radiotherapy/radiosurgery without concern for radiation-related optic neuropathy.
Pearls and Pitfalls
- Extracavernous tumor resection and conservative lateral intracavernous resection are reasonable strategies for handling meningiomas of the region.
- Preoperative palsy caused by tumor compression on CNs III, IV, and VI can improve after effective tumor decompression. The extent of tumor resection is not necessarily related to the chance of recovery of CN function. Therefore, the principles of conservative tumor removal and CN decompression are wise strategies for patients with compromised preoperative CN function.
Contributors: Andrew R. Conger, MD, MS, and Benjamin K. Hendricks, MD
References
Couldwell WT, Cole CD, Al-Mefty O. Patterns of skull base meningioma progression after failed radiosurgery. J Neurosurg. 2007;106:30-35.
Demonte F, Al-Mefty O. Cavernous sinus meningioma management with carotid preservation, in: Eisenberg MB, Al-Mefty O (eds): The Cavernous Sinus: A Comprehensive Text. Philadelphia: Lippincott Williams and Wilkins, 2000, 251-261.
Dunn I, Al-Mefty O. Cavernous sinus meningiomas, in: Demonte F, McDermott M, and Al-Mefty O (eds): Al-Mefty's Meningiomas. 2nd ed. New York: Thieme, 2011, 235-247.
Hirsch WL, Sekhar LN, Lanzino G, Pomonis S, Sen CN. Meningiomas involving the cavernous sinus: Value of imaging for predicting surgical complications. AJR Am J Roentgenol. 1993;160:1083-1088.
Johnson MD, Powell SZ, Boyer PJ, Weil RJ, Moots PL. Dural lesions mimicking meningiomas. Human Pathol. 2002;33:1211-1226.
Kawase, T, Van Loveren, H, Keller, J, and Tew, J. Meningeal architecture of the cavernous sinus: Clinical and surgical implications. Neurosurgery. 1996;39:527-534.
Larson J, Van Loveren HR, Balko G, and Tew JM Jr. Evidence of meningioma infiltration into cranial nerves: clinical implications for cavernous sinus menigiomas. J Neurosurg. 1995;83:596-599.
O'Sullivan MG, van Loveren HR, Tew JM Jr. The surgical respectability of meningiomas of the cavernous sinus. Neurosurgery. 1997;40:238-244, discussion 245-247.
Rhoton A. The cavernous sinus, the cavernous venous plexus, and the carotid collar. Neurosurgery. 2002;51:S1-375-410.
Sindou M, Wydh E, Jouanneau E, Nebbal M, Lieutaud T. Long-term follow-up of meningiomas of the cavernous sinus after surgical treatment alone. J Neurosurg. 2007;107:937-944.
Tagle P, Villanueva P, Torrealba G, Huete I. Intracranial metastasis or meningioma? An uncommon clinical diagnostic dilemma. Surg Neurol. 2002;58:241-245.
Related Materials
Available Through the Atlas
-

Microsurgical resectability, outcomes, and tumor control in menin...
-
Stereotactic radiosurgery providing long-term tumor control of ca...
-
Operative management of tumors involving the cavernous sinus
-
Extradural temporopolar approach to lesions of the upper basilar...
-

The surgical resectability of meningiomas of the cavernous sinus
-
Analysis of treatment outcome after stereotactic radiosurgery for...
-
Sphenoorbital meningiomas: Surgical limitations and lessons learn...
-
Meningiomas involving the cavernous sinus: Histological factors a...
-
Long-term follow-up of meningiomas of the cavernous sinus after s...
-
Management of meningiomas en plaque of the sphenoid wing
-
Long-term outcomes of Gamma Knife surgery for cavernous sinus men...
-
A combined frontotemporal and lateral infratemporal fossa approac...
-
Anterior clinoidal meningiomas: Functional outcome after microsur...
-
Decompression of cavernous sinus meningioma for preservation and...
-
Factors affecting outcome following treatment of patients with ca...
-
Posterior petrous meningiomas: 82 cases
-
Long-term results with exophthalmos in a surgical series of 30 sp...
-
Sphenoorbital meningioma: Surgical technique and outcome: Clinica...
-
True petroclival meningiomas: Results of surgical management. Cli...
-
Meningiomas involving the optic canal: Pattern of involvement and...
-
Neuroophthalmological evaluation after Gamma Knife surgery for ca...
-
Giant anterior clinoidal meningiomas: Surgical technique and outc...
-
The treatment of cavernous sinus meningiomas: Evolution of a mode...
Unavailable Through the Atlas
-
Microsurgical Anatomy and Approaches to the Cavernous Sinus
-
The cavernous sinus, the cavernous venous plexus, and the carotid...
-
Surgical Approaches to the Cavernous Sinus: A Microsurgical Study
-
Long-term follow-up of patients with meningiomas involving the ca...
-
Cavernous sinus hemangiomas: A series, a review, and an hypothesi...
-
The results of surgery for benign tumors of the cavernous sinus
-
Large sphenoid wing meningiomas involving the cavernous sinus: Co...
-
Meningiomas involving the optic nerve: Technical aspects and outc...
-
Meningiomas of the space of the cavernous sinus
-
Medial sphenoid wing meningiomas: Clinical outcome and recurrence...
-
Surgical Treatment of Meningiomas Involving the Cavernous Sinus:...
-
Cavernous sinus meningiomas - What is the strategy: Upfront or ad...
-
Cranial base surgical techniques for large sphenocavernous mening...
-
Gamma knife surgery of meningiomas involving the cavernous sinus:...
-
Surgery of extra-axial tumors of the cerebral base
-
Medial sphenoid ridge meningiomas: Classification, microsurgical...
-
Management of intracranial meningiomas secondarily involving the...
-
Meckel's cave tumors: Relation to the meninges and minimally inva...
-
En plaque sphenoid wing meningiomas: Recurrence factors and surgi...
-
Extended middle fossa resection of petroclival and cavernous sinu...
-
Does prior microsurgery improve or worsen the outcomes of stereot...
-
Clinical characteristics and surgical outcomes of patients presen...
Please login to post a comment.