Nuances in AVM Resection



This is a preview. Check to see if you have access to the full video. Check access
Technical Principles of AVM Surgery
Please note the relevant information for patients suffering from an arteriovenous malformation is presented in another chapter. Please click here for patient-related content.

Atlas Choice Tapered Pattie Collection
Low-profile for maximal visualization and protection
Tapered shape designed for retractorless surgery
Unparalleled flexibility and non-stick features
Arteriovenous malformations (AVMs) are an important cause of morbidity and mortality among neurosurgical patients, usually due to hemorrhage, but also because of refractory seizures and focal neurologic deficits.
Management options for AVMs vary from microsurgery alone or in conjunction with or without adjunctive embolization and/or radiosurgery. Alternative options include radiosurgery as a standalone option. Large and complex lesions may be best managed via observation.
The specific technical nuances for excision of each AVM subtype will be discussed in the following chapters. The current chapter will review the general principles applicable to all AVMs and should be consulted before reviewing the subsequent chapters.
Please also refer to this article published in the WORLD NEUROSURGERY about my personal perpectives on AVM surgery.
Patient Positioning
As previously discussed in the Cranial Approaches volume, thoughtful positioning of the patient during surgery can facilitate resection by allowing the use of gravity retraction.
Head position is planned with the cranial venous return in mind, keeping the patient’s head just above the level of the heart, and the neck slightly extended while avoiding extreme rotation of the head to one side. These considerations prevent intracranial venous hypertension, which can be problematic for cranial surgery in general and in AVM surgery in particular.
Common mistakes during patient positioning include failure to use free surfaces to access the lesion and maximize gravity retraction. As a result, fixed retractors may become necessary, risking cortical injury and potentially increasing morbidity.
Due to risk of intraoperative bleeding and technical challenges associated with AVM surgery, the operative corridor has to be generous and provide numerous working angles that are flexible for timely handling of subcortical bleeding. Finally, patient positioning should take into account operative routes that will minimize any risk to the venous drainage of the AVM and facilitate early access to the feeding vessels.
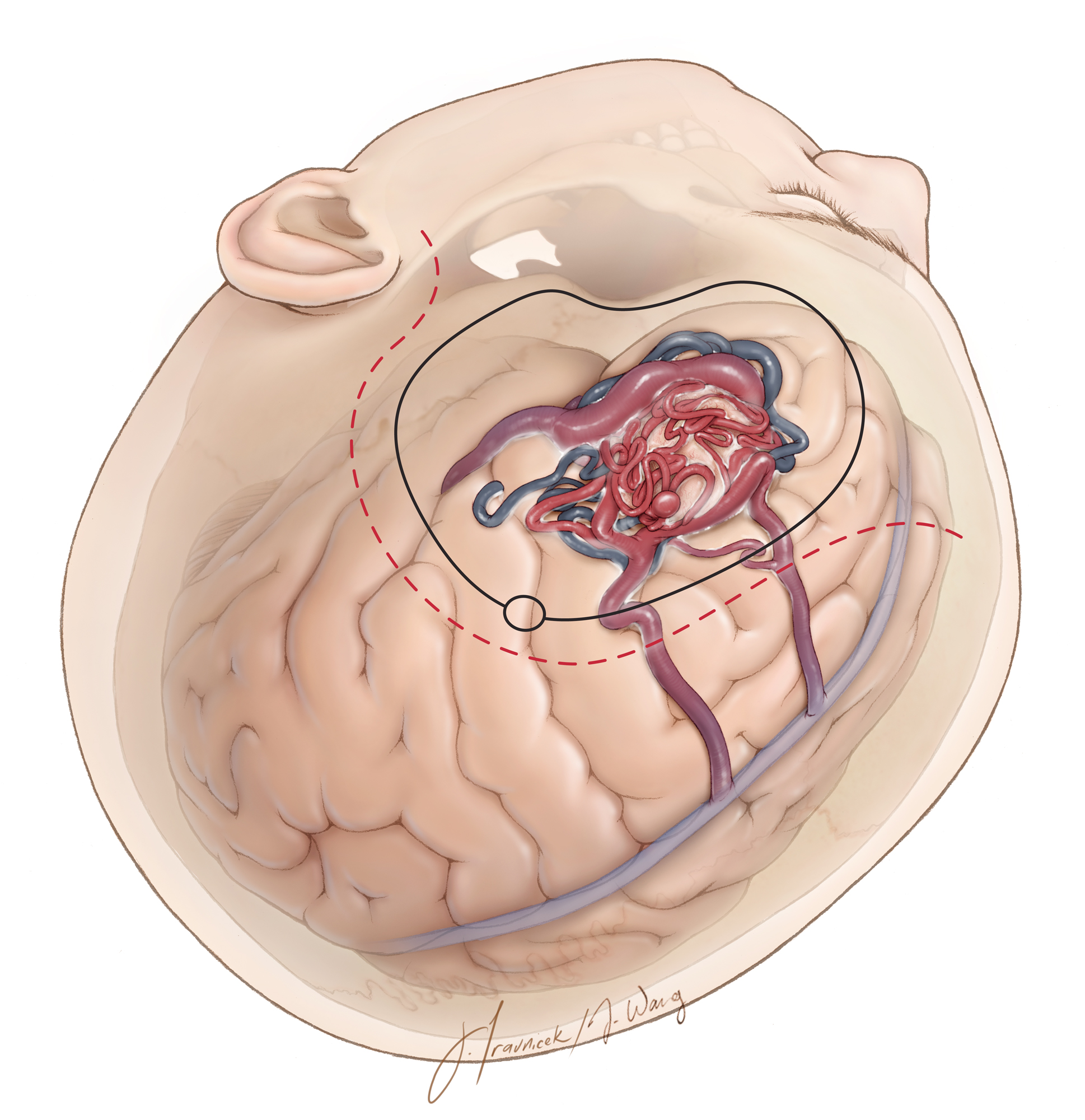
Figure 1: Head positioning as well as incision and craniotomy outlines for a typical left frontal AVM is demonstrated. Note the generous exposure of the peri-lesional brain.
Craniotomy
I use neuronavigation or intraoperative image guidance based on magnetic resonance imaging or preferably CTA angiogram data to achieve a wide craniotomy and expose the AVM nidus, its associated feeding arteries and draining veins, and a region of normal brain surrounding the AVM. Craniotomies for AVMs are not minimally invasive and should be generous.
When possible, the craniotomy is planned to provide exposure and early opening of cerebrospinal fluid (CSF) cisterns to relax the brain. If this is impractical, I install a lumbar drain to gradually drain CSF during the craniotomy to provide brain relaxation. A greater number of burr holes and short passes of the craniotome decrease the risk of injury to dilated draining veins that may be traveling within the parasagittal dural leaves and along the venous lakes.
Any violation of the dura during the use of the footplate increases the risk of unintended injury to the draining veins. The avoidance of this complication can be difficult because the engorged draining veins within the dural leaves are often large enough to erode the inner table of the calvarium. The use of the lumbar CSF drainage can facilitate thorough dissection of the decompressed dura away from the inner surface of the calvarium before the footplate is employed.

Figure 2: Following the craniotomy, a wide durotomy unveils the brain while protecting the underlying vessels. The dura is opened slowly and meticulously because scarring from previous hemorrhage(s) may cause it to be adherent to the underlying AVM or an associated vessel. Tearing of a draining vein this early in the operation can be disastrous because of heavy bleeding and the likelihood of occluding the draining vein while attempting to control the hemorrhage.
GENERAL STEPS AND NUANCES OF TECHNIQUE FOR AVM RESECTION
There are certain universal mandatory steps during microsurgical excision of every AVM. It is best to adhere to these principles as much as possible. Violating any of these principles or their specific order has caused me many misgivings.
The following are general principles that will be elaborated upon in the individual chapters of each subtype of AVMs.
Step 1: Thee-Dimensional Understanding of the Malformation
I study every sequence of the preoperative angiogram and MR images and familiarize myself with a well thought-out strategy. The feedings vessels and their morphology, location, and serpentine routes are memorized. The surface landmarks, large draining veins, and embolic material are used as guides to localize feeding arteries. I map the specific border of the AVM containing the predominant feeding arteries so the nidal dissection and disconnection begins there.
CT angiogram scans and MR images are used to plan the dissection strategy in relation to the hematoma cavity. Functional cortices are anatomically mapped in relation to the nidus and the hematoma. The locations of the deep white matter feeders are noted. I prefer to use CT angiogram sequences for intraoperative navigation because of its high-resolution vascular anatomy in relation to brain surface landmarks.

Figure 3: A large right-sided temporoparietal convexity AVM is demonstrated. The MCA branches along the anterior pole of the lesion are the primary feeders and should be disconnected first. The embolic materials mark the superior and the anterior borders of the AVM (lateral ICA arteriogram-left upper image). The primary vein is travelling supraposteriorly. The MR image (right upper) discloses the vicinity of the lesion to the functional cortices and ventricular chambers, and locates the deep white matter feeders to the trigone. CT angiogram sequences (lower images) provide information regarding the vascular anatomy (including the deep draining vein) in relation to the parenchyma and skull landmarks for intraoperative planning.
Giant/Large Temporoparietal AVM
Ruptured border of the AVM is accessed first to decompress the hematoma cavity and relax the brain. On the other hand, the border of the AVM facing the eloquent cortex is handled last when the AVM is mostly defeated.

Figure 4: The general angioarchitecture of a convexity AVM is illustrated. Feeding vessel aneurysms should be distinguished from nidal aneurysms. Large feeding arteries hide within the peri-AVM sulci and require patient arachnoid dissection for their exposure. The primary draining vein can wrap around the deeper parenchymal sections of the AVM and should be carefully protected during AVM disconnection. Indiscriminate coagulation of the nidus and the vein is prohibited. White matter feeders provide the most challenge for their control and lack robust muscular walls.
Step 2: Generous Exposure and Preparing for the Battle
I plan flexible working angles via appropriate patient positioning. Gravity retraction and wide arachnoid dissection allow dynamic retraction using the suction device to protect vital normal anatomy against fixed retractor blades.
The craniotomy should not be minimally invasive, but generous to expose every arterial feeder and all the draining veins. The dura should be opened widely so that normal structures surrounding the AVM can be identified. I do not plan the size of the craniotomy according to the size of the angiographic nidus of the AVM.
I do pay special attention to the dissection planes where deep white matter feeders (i.e., lenticulostriate arteries) can lead to uncontrolled torrential bleeding. I assure myself adequate space and ergonomic working angles to handle the tough moments during disconnection of the deep white matter feeders.
Step 3: Managing the Feeding Arteries
I open the fissures and sulci to identify the feeding arteries but leave the veins alone.

Figure 5: Patience of the surgeon is a virtue during exposure of feeding vessels and subarachnoid dissection (upper illustration). The arachnoid bands over the AVM are commonly thickened. I favor the use of jewelers’ forceps for grabbing the edges of the arachnoid bands and gently tearing the thickened superficial arachnoid layers to unveil the cortical feeding vessels (lower intraoperative photo). Occasionally it is impossible to differentiate clearly between an artery and a vein because of high flow arterialization of the vein. This distinction may become more apparent at the end stages of AVM dissection and excision when the arterialized veins turn blue and demonstrate their true identity.
If an early and clear understanding of the character of a vein or an artery is important for operative planning and its disconnection, I attempt a brief trial occlusion of the feeding artery or draining vein by gently squeezing the vessel using a pair of forceps or a temporary aneurysm clip (the “temporary occlusion” test). If engorgement of the AVM occurs, the occluded vessel is certainly an important draining vein and should be kept intact until the end of AVM disconnection. Intraoperative fluorescence angiography can also be effective in demonstrating the timing of flow and the character of the vessel.
A draining vein at the surface may herald the path to a deep lesion without any surface presentation, whereas other subcortical AVMs require detection of more subtle surface cues such as small arterialized veins or mildly dilated arterial feeders, either of which can be traced down to a sulcus and ultimately to the AVM nidus.

Figure 6: The small and medium sized cortical and pial feeding arteries (arterioles) coagulate readily and should be efficiently handled without any major concern for their lack of bipolar coagulation and uncontrollable bleeding as seen with the deep white matter feeders. There is no reason not to markedly speed up the dissection process when it comes to manipulating these feeding arterioles that own robust walls.

Figure 7: The surgeon should not overzealously sacrifice en passage vessels along their cortical and pial surfaces. Microclips are useful to collapse large terminal feeding arteries before their coagulation where they enter the nidus. These large diameter arteries have thickened walls and occasionally may not readily respond to or collapse with bipolar electrocautery alone.

Figure 8: The feeding arterioles and arteries are “corkscrew,” dysmorphic, and at times distended (green arrow), as compared with normal suppliers to the adjacent brain. These configuration differences can help the operator differentiate AVM feeding vessels from branches of the en passage vessels (red arrow).

Figure 9: In contrast to cortical arterioles, the small caliber deep white matter feeders have little elastic tissue and smooth muscle layers, and therefore do not constrict upon bipolar coagulation (upper images). They may continue to bleed vigorously, retract into the white matter and cause intracerebral hemorrhage in an area of the brain away from the AVM. Deep white matter feeders must be pursued and isolated via removal of a small amount of white matter immediately around them (left lower image) so that their more proximal segment with relatively normal walls, away from the nidus, is preferably coagulated or clip ligated (right lower image). This maneuver is critical for avoiding unnecessary morbidity associated with AVM surgery. Packing the bleeding site with hemostatic materials will not attain hemostasis, only provides the surgeon with a false sense of security, and leads to brain swelling because of remote intracerebral hematomas.
Managing Difficult Deep White Matter Feeders

Figure 10: The use of microclips for the larger cortical feeding vessels and small white matter feeders should be minimized as much as possible as the clips can be inadvertently dislodged. As demonstrated, their bulk interferes with the next operative maneuvers. Bipolar coagulation of the white matter feeders is the most practical method to control their bleeding, however; clips should be used if bleeding continues.
Radiosurgery transforms delicate-walled white matter feeders to readily coagulable vessels. The gliotic white matter changes that are induced by radiation provide a clue regarding thickening of the wall of the fine white matter vessels.
Step 4: Strategic Circumdissection
Dissection should proceed in a circumferential or spiral-like fashion to expose every aspect of the AVM toward its apex, which is often located near the ventricular ependyma. I use intraoperative navigation based on CTA for guiding the superficial pial incisions and deep white matter dissection where the nidus margins are not very clear. I often can find the nidus and maintain the dissection outside its borders.

Figure 11: I use the natural fissures and sulci and promote circumdissection through these planes. The surgeon should not work through uneven planes and deep holes as unexpected bleeding will be difficult to control. Occasionally the feeding artery leaves the sulci, and I must dissect through subpial planes or enter the adjacent gyrus. Entry into the nidus is strictly avoided.
Each AVM has its own individual angioarchitecture and borders. The strategic steps for microdissection include: 1) subarachnoid/pial dissection, 2) parenchymal dissection, 3) ependymal dissection, 4) inspection to ensure complete nidus disconnection, and finally primary vein sacrifice, leading to 5) AVM removal.

Figure 12: The basic steps in AVM resection are demonstrated. The AVM was only apparent on the surface based on a questionable feeding artery versus draining vein leading to the subcortical AVM (upper left image-arrow). Pial dissection was performed (upper right photo). Subarachnoid dissection revealed an en passage artery (middle left image-arrow). Parenchymal disconnection exposed the borders of the nidus (middle right photo-arrows); the identity of the cortical vessel (blue arrow) is still unknown, however, it is carefully preserved. Embolized vessels were found and assisted with white matter dissection (lower left photo). The small draining veins were sacrificed after complete AVM disconnection. The initial cortical vessel (upper left image-red arrow) was finally identified as an en passage artery that was spared (lower right image).
I avoid any coagulation of the nidus before its complete disconnection. If a bleeding defect in the nidus wall is apparent as I inadvertently wander too near the nidus lobules that project into the brain, I place a very small piece of thrombin-soaked cotton to plug the defect. Gentle tamponade and patience will seal the defect. Aggressive coagulation of the nidus will acutely alter its internal hemodynamics and intraluminal flow pattern, leading to its rupture and brain swelling.
Step 5: Protecting the Dominant Vein
The veins are great superficial landmarks to transpose and navigate the preoperative angiographic findings onto the operative field. The main draining vein (sometimes multiple main draining veins) should be the last part of the operation. These veins should be preserved until the entire nidus is disconnected from all of its feeding arteries. After the AVM disconnection, the veins become darker. If this change does not occur or if temporary clipping of the vein leads to nidus swelling, the surgeon should search for hidden, residual feeders, usually located near and underneath the vein(s).
If I inadvertently tear a main draining vein before large feeding arteries are encountered and sacrificed, I do not occlude the vein, because this maneuver will lead to sudden AVM rupture and immediate brain swelling. I allow the vein to bleed while I efficiently find the feeding arteries at the nidus and disconnect them. A “commando” operation is necessary at this point, and the surgeon must remain calm, decisive, and in control. Successful performance of this critical and life-threatening step is required for the maturation of every AVM surgeon.
There are primary veins and secondary veins. I designate the primary vein preoperatively based on the angiographic findings of the vessel that has the largest diameter and carries the most flow out of the AVM. The secondary veins may be sacrificed before complete AVM disconnection as long as the flow into the nidus has been sufficiently reduced through stepwise circumferential dissection. The exclusion of some of the secondary veins is often necessary for me to mobilize the AVM and disconnect deep and hidden feeding arteries.

Figure 13: The “temporary occlusion” test is necessary before the primary or secondary veins are transected. If AVM swelling is encountered upon temporary vein occlusion, additional devascularization of the nidus is necessary before venous sacrifice.
The primary vein may wrap around the deeper sections of the nidus before the vein reaches the surface. One must avoid the temptation to coagulate the vein during the parenchymal steps of dissection to create more space. Ideally, any bleeding from the deeper portions of the vein should be covered with a piece of cotton and controlled with gentle tamponade; aggressive indiscriminate cautery leads to more bleeding and risks a rupture.
Step 6: Efficient Excision of the AVM
I analogize the final steps in AVM removal to landing a plane under turbulent weather conditions. One cannot fear the storm and avoid landing. The final steps of dissection for large AVMs often involve some bleeding from the resection bed and the nidus. The surgeon must remain in control and remember that timely removal of the AVM is the best method to control the bleeding.
AVMs that are near the ependyma incorporate ependymal and plexal feeding vessels, despite nonremarkable angiographic findings near the periventricular region. Therefore, to avoid recurrence of AVMs with periventricular components, especially in pediatric patients, I extend the circumdissection to the level of the ventricle and disconnect the ependymal/plexal feeding vessels.
I have unfortunately been surprised in a number of cases when I attempted to disconnect a “vein” at the depth of resection cavity when actually I truncated a deep section of the AVM nidus. Careful inspection of the ventricular wall can avoid these errors and the delayed/future risk of hemorrhage or AVM recurrence.
Choroidal arteries are more easily controlled using bipolar electrocautery, although if these vessels are difficult to visualize behind the AVM nidus, clips can be applied. If a choroidal feeding artery retracts on coagulation, avulses and gets away, it can cause unrecognized bleeding into the ventricle, risking brain herniation. The ependymal arteries can be a significant source of feeding vessels to the AVM. Therefore, unexpected brain herniation at this step of the operation should alert the operator to examine the ventricle to evacuate the blood and deal meticulously with the bleeding ependymal feeding vessels.
I have also been surprised by the presence of functionally significant feeding arteries that reside next to a primary draining vein. My compulsive actions to protect the vein often leaves these feeding vessels unnoticed and prevents the vein from turning blue. Therefore, if the entire AVM is disconnected except the primary draining vein, but the vein is still red, a hidden feeding artery in close proximity of the vein should be sought and severed.

Figure 14: Finally, the veins are clipped, coagulated and transected. The resection bed should be meticulously inspected for possible residue of the nidus. Note the preservation of the en passage artery on the right side of the resection cavity.
In my opinion, intraoperative angiography is mandatory to ensure complete obliteration of arteriovenous shunting in most medium to large size AVMs. Subtle “luxury perfusion” associated with minor arteriovenous shunting, away from the nidus, especially in the pediatric patients, does not warrant an aggressive pursuit and should be monitored long-term.
Following angiographic confirmation of AVM removal, complete hemostasis is secured. The patient’s mean arterial pressure should be raised up to 15-20 mm/hg above the baseline level and maintained for 10 to 15 minutes. Any bleeding is suspicious for residual AVM nidus and indicates a high risk of postoperative hematoma development. The only method to achieve hemostasis is to remove the residual AVM.
Coagulation of the friable white matter is minimized, as this maneuver will lead to more bleeding. Multiple rounds of irrigation fluid and patience are needed to achieve meticulous hemostasis.
At the end of surgery, the patient’s systolic blood pressure should be maintained slightly (10-20%) below the baseline levels for 24 hours following the operation. The results of the CT scan on the first postoperative day determine if the blood pressure parameters can be slowly liberalized.
Additional Technical Considerations
The following images further summarize my techniques for AVM removal. This left-sided basal frontal AVM illustrates the relevant details.

Figure 15: The technical nuances for resection of a left basal frontal AVM is demonstrated (first two rows). Note the osteotomy over the orbital roof to provide an adequate inferior-to-superior operative trajectory without excessive frontal lobe retraction (third row). Subarachnoid dissection, anterior to the Sylvian fissure, allowed disconnection of predominant AVM feeders from the MCA. A prominent feeding artery (red arrow), as expected, hid next to the draining vein(s)(purple arrow). The nidus was skeletonized (fourth row). The draining vein was preserved but mobilized to provide access to the deep portions of the AVM. Next, the deep white matter feeders were found and sacrificed (fifth row). Temporary occlusion of the primary draining vein revealed adequate AVM disconnection. The AVM was removed and all the cortical veins were noted to turn dark blue (bottom row).
Postoperative Considerations
The patient is admitted to the intensive care unit after surgery and is closely observed for evidence of postoperative bleeding. After difficult cases, large AVMs, presence of intraoperative swelling, or any case that causes concern for postoperative hemorrhage, the patient remains intubated and sedated overnight to prevent the blood pressure spikes that often accompany coughing and gagging during extubation.
A CT scan and angiogram is obtained on the first postoperative day. If any AVM remnant is demonstrated, the patient is returned for a reoperation immediately or as soon as the patient is deemed safe to return to surgery. Pediatric AVMs are notorious for their recurrence, partly due to their noncompact nidus, and must undergo surveillance imaging for years after surgery.
Complication Avoidance and Management
Resection or embolization of AVMs can be marred by many complications, including neurologic deficits from overly aggressive dissection or ischemic infarcts, seizures, hydrocephalus, and infection; however, 3 complications deserving specific consideration are intraoperative rupture, postoperative hemorrhage, and postoperative edema.
Intraoperative AVM rupture is a potentially disastrous consequence of premature occlusion of one or more major draining veins. This event often occurs during attempts to regain hemostasis after the draining vein is injured or by kinking of the vein while the nidus is held under fixed retraction. This can also occur during attempted embolization of high-flow fistulas. All of these unfortunate moments are more likely to occur in the event of heavy bleeding and pressured decision-making, underscoring the importance of maintaining hemostasis throughout the dissection process. For further details, please refer to the Chapter on Intraoperative Rupture and Complication Management.
Residual AVM nidus can lead to bleeding within the adjacent normal brain and intraoperative brain swelling. Once a significant portion of the AVM outflow has been compromised, the nidus swells, arterial feeders engorge and become less responsive to coagulation, and areas of the nidus and brain begin to spontaneously bleed. At this point, careful, methodical dissection is no longer an option, and an operation ensues that I refer to as the “commando resection.”
The impending AVM rupture necessitates thoughtful, decisive, and deliberately aggressive mobilization of the nidus and coagulation of the remaining larger arterial feeders. Smaller feeders near the base of the AVM are initially ignored as the nidus is removed. Next, with the nidus out of the way, the cavity is rapidly examined for active bleeders and hemostasis is re-established. This technique often requires dissecting into the white matter to expose a length of these small, friable, deep perforating vessels, followed by their clip ligation. Because of its increased risk of morbidity, the commando resection is clearly not ideal, but it is essential under these circumstances to prevent rupture of the AVM and potentially catastrophic brain herniation and blood loss.
Severe edema and hemorrhage are the two postoperative complications that occur most often after resection or embolization of large and high-flow AVMs. The exact etiology of these complications remains unclear, but is most likely a result of altered hemodynamics in the wake of AVM manipulation.
Two explanations have been proposed. The phenomena of “normal perfusion pressure breakthrough,” asserts that the arterioles surrounding an AVM are usually exposed to low perfusion pressures and are maximally vasodilated. As a result, these arterioles are unable to immediately autoregulate upon restoration of normal perfusion pressures following AVM resection. This alternation leads to edema and hemorrhage within the surrounding brain. The second explanation suggests that obstruction of venous outflow and stagnant arterial input within the tissues surrounding the resection cavity cause edema, hypoperfusion, ischemia, and hemorrhage.
Regardless of the cause, these complications are more common during resection of larger AVMs associated with high-flow shunting; and therefore appropriate measures for postoperative blood pressure control should be taken. These adverse effects can also be minimized or avoided by gradual embolization of portions of the AVM before surgery to allow the surrounding brain to accommodate to the hemodynamic changes that ensue after sudden AVM resection.
Managing the altered hemodynamics in this staged manner decreases the incidence of these postoperative complications. If edema or hemorrhage develops postoperatively despite meticulous blood pressure control, it can be managed medically with hypertonic therapies or, if necessary, a ventriculostomy to drain cerebrospinal fluid and decrease intracranial pressure. Rarely, operative evacuation of the hematoma or decompressive craniectomy is mandatory; the resection cavity should be examined with an angiogram or intraoperatively for residual nidus.
Personal Advice
I believe surgery should be conducted during the acute phase of hemorrhage on patients who present with a ruptured AVM and are in good neurological condition. This allows the patient to recover from the temporary consequences of the hemorrhage and the surgery simultaneously.
An acute hemorrhage provides reasonable dissection planes, but chronic gliosis from a previous hemorrhage can potentially be more challenging to deal with. Furthermore, acute evacuation of the clot and AVM often facilitates faster recovery from the mass effect of the intracerebral hemorrhage. However, acute cerebral edema, as a result of AVM rupture, causing neurological decline, requires delayed surgical care. Edematous brain is friable and vulnerable to injurious operative maneuvers.
Packing the bleeding points from the AVM’s white matter feeders during the parenchymal phase of dissection almost never works and leads to increased brain tension because of occult or remote foci of intracerebral hemorrhage. I recommend addressing the bleeding source immediately and managing it patiently. It is not advisable to leave one bleeding site and cause bleeding at another site by diverting attention elsewhere.
Removal of the AVM will lead to hemodynamic alternations in the surrounding vascular territories; these alterations lead to gradual regression of feeding vessel aneurysms. Therefore, difficult-to-reach aneurysms are left alone and the attention is directed to the excision of the AVM. However, I attempt clip ligation of the more accessible aneurysms (MCA bifurcation) during microsurgical removal of the peri-Sylvian AVMs.
Pediatric AVMs are a different entity than those of adults. They are frequently immature and partly diffuse AVMs whose definite borders are not easily identifiable, even on a preoperative angiogram. These diffuse lesions have a substantial risk of recurrence, even after their angiographically-proven gross total resection. I have faced multiple instances when the post-resection intraoperative angiogram confirmed gross total resection of a pediatric AVM, but the postoperative angiogram revealed a newly identified small early draining vein, sometimes slightly remote from the resection cavity. An aggressive approach to these “minor” arteriovenous shunts may not be warranted, even though their natural history is not clearly defined.
AVM surgery defines the best of us as microneurosurgeons. One cannot remain hesitant, timid, and indecisive. The surgeon must direct the operation efficiency and fluently. Fatigue becomes an important factor later in the procedure and can dramatically affect the outcome.

Figure 16: I do not routinely embolize AVMs before surgery (left image). In fact, I believe embolization of cortical pedicles (often easily managed during surgery) leads to an increase in the functional role of daunting white matter perforators (right image). This phenomenon is founded on the principle that each AVM will persist in its role of arteriovenous shunting. If the large pedicles are lost, the AVM will find a way to shunt through the white matter feeders that are often inaccessible for embolization.
However, selective embolization of some of the arterial pedicles is advised if these pedicles are not easily accessible early in surgery (i.e., P2 feeders). The accessible pedicles should be left alone to avoid the AVM’s proliferation of white matter feeders. It is important that the planning for the embolization be conducted through direct communication between the neurosurgeon and the endovascular interventionalist.
Even using perfect techniques, the surgical field of an AVM cannot and should not be “too dry.” In other words, some degree of minor bleeding should be expected and tolerated, especially around the end of the operation, just before the AVM is extracted. This “pre-extraction storm” should not be feared and avoided. Resection of an AVM has been compared to flying a plane. The landing is always going to be somewhat “bumpy.” We should however avoid the turbulence in the cruising altitude as much as possible.
I have a high tolerance for controlled intraoperative bleeding and can gauge the fine line when a controllable bleeding may lead to an uncontrollable torrent. This understanding has lead to efficient resection of large AVMs without a need for staged operations.
The critical ingredients that define a great AVM surgeon include: 1) instantaneous translation of 3D anatomy to intraoperative findings, 2) appropriate surgical judgment refined by humility and “surgical intuition,” 3) manual dexterity, 4) endurance, 5) mental toughness, 6) calm composure in dealing with disasters, and ultimately, 7) experience.
There is no place to prepare for the battle when you are fighting it. The AVM surgeon must intimately understand the roadmaps of the AVM and its difficult territories before commencing the operation. The process of AVM resection should be executed without hesitation, but gracefully. Despite torrential bleeding, the operator is in control and has undoubtedly convinced the team that no matter how difficult the moment, he or she can prove his or her commanding omnipresence.
AVM surgery tests not only the operator’s technical prowess, but also the operator’s perseverance and efficiency. This phenomenon distinguishes AVM surgery from all other surgeries in our profession.
Related Materials
Available Through the Atlas
-
Endovascular and microsurgical treatment of cerebral arteriovenou...
-

Microsurgical treatment of arteriovenous malformations in pediatr...
-
Brainstem arteriovenous malformations: anatomical subtypes, asses...
-
Management of perisylvian arteriovenous malformations: a retrospe...
-
Intraoperative arteriovenous malformation rupture: causes, manage...
-
Microsurgery for cerebral arteriovenous malformations: postoperat...
-
Challenging Dogma in Arteriovenous Malformation Surgery: Personal...
Unavailable Through the Atlas
Please login to post a comment.



Comments: